Vienici a trovare
Old-fashioned or renewed art of medical orthodontics?
We often witness the promotion of a business model to practice modern orthodontics that we can call appliance-centered orthodontics (ACO).
An evident example of ACO is the sale and advertising of clear aligner treatment, based only on the patient’s cosmetic demand for straightening their teeth using invisible appliances and not on clinical necessity and aptness. These appliances are supplied by the companies to the provider doctors, who deliver the devices to the consumers.
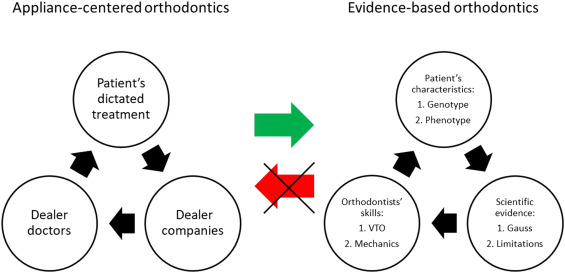
Diagram of the two models of orthodontic clinical practice: the evidence-based orthodontics (EBO) model and the ACO model.
Concerning this practice model, several issues have been raised recently:1
- Sometimes doctors are bypassed and business promotion is conveyed directly to the patients; this may stimulate the demand for do-it-yourself orthodontics, a growing phenomenon.
- The perspective of dealer companies is to increase their profits as they have to respond to their investors. Therefore, a commercial relationship between dealers and consumers is usually promoted. Instead, a relationship based on mutual trust should be developed.
- The reduced effectiveness for some types of dental movements, shown by plastic appliances compared with conventional treatments,2 compels us to accept outcomes with a reduced quality if a thorough assessment of treatment indications is not performed.
- The risk of acquiescing to the patient’s dictated treatment even in patients showing reduced outcome predictability; the latter scenario exposes the dealer doctor (i.e., the doctor who is providing the appliance) to possible litigations and refunds. According to the author, the definition of dealer doctor is based on the fact that in some patients, the choice of the appliance could be based on the relationship that the clinician has with the dealer company, even unconsciously or involuntarily (discounts, marketing, etc) rather than on the real clinical indications.
- The production of these appliances results in excessive amounts of plastic waste, and disposal presents an urgent problem.
The evergreen concept of evidence-based orthodontics is based on three pillars (Fig): patient characteristics, scientific evidence, and specialist skills. All these pillars contribute to achieving treatment goals and improving oral health–related quality of life. These goals should always aim (1) to favor facial esthetics and smile harmony, (2) to obtain correspondence between the centric occlusion and centric relation, (3) to correct the malocclusion, (4) to keep the periodontal tissues healthy, (5) to obtain long-term results.
Patients’ characteristics
Traditionally, this pillar is described as the need for the clinician to follow the patient’s expectations and preferences.3 Moreover, the author would like to add that because patients show a personalized response to orthodontic therapy because of their genotype and phenotype, deep knowledge in biology, growth and development, periodontics, and tooth decay, is essential to apply predictable and safe mechanics to reach the visualized treatment objectives (VTO).
Scientific evidence
Deep knowledge of the available scientific evidence helps to identify the proper treatment strategy and appropriate mechanics to reach treatment goals. Moreover, knowing and understanding the limitations and the advantages of different appliances and techniques, as demonstrated by sound scientific literature, and being up-to-date with the technical and scientific evolution, will help the clinician provide real health care rather than being a simple dealer doctor. However, this pillar shows two main limitations: (1) the differences among people, even in study samples showing normal data distribution. This variability is located at the extremities of the Gaussian curve; (2) the difficulties in designing and performing randomized clinical trials for ethical reasons or lack of funds. These limitations imply that data must be interpreted with caution and orthodontists must be able to translate scientific data into clinical practice.
Specialist skills
The orthodontist needs both diagnostic and treatment skills. During the diagnostic stage, the specialist must be able to visualize the reachable goals and mechanics needed to correct the malocclusion through VTO. During the treatment phase, the specialist must be able to move teeth according to the VTO and monitor the progress toward the desired results. If the pictures taken during treatment progress show an unfavorable trend, a new VTO with the progress data is necessary. The following list is a decalogue of the orthodontists’ skills required to approach every patient appropriately:
- To visualize goals in harmony with boundaries and the face.
- To obtain the desired root movement predictably.
- To exploit the favorable biological timings.
- To manage the anterior limit of the dentition.
- To manage the occlusal plane in various types of malocclusion.
- To manage the temporomandibular joints and the myofascial function.
- To refine the case at best.
- To obtain a beautiful smile.
- To fix the maxillary incisor exposure.
- To manage long-term stability.
Therefore, from this perspective, the orthodontist should be considered an artist who visualizes the “artwork before painting or sculpting” and creates with proper instruments: the knowledge, expertise, and modulation of single or coupled forces.
In this evidence-based orthodontics perspective and contrast with the ACO model, a skilled orthodontist will be considered a renewed medical specialist of a renewed practice model that the author likes to call the Art of Medical Orthodontics (AMO).
The renewed AMO concept is also coherent with the original Art of Medicine mentioned in the Hippocratic Oath. AMO reaffirms the doctor’s centrality to obtain orthodontic health and, at the same time, to meet the patient’s expectations. In a Society that values appearance and consumerism the most and the risk of being swallowed up by ACO-like models, we orthodontists shall remember we are health providers in the first place and always aspire to an AMO model.
AMO principles should be the fundamentals principles to build renewed orthodontics in the digital era because:
Medicine is of all the Arts the most noble; but, owing to the ignorance of those who practice it, and of those who, inconsiderately, form a judgment of them, it is at present behind all the arts.
REFERENCES
- F. Ciuffolo
The key factors for future orthodontic prosperity: a commentary paper
APOS Trends Orthod, 11 (2021), pp. 169-173
View PDF CrossRef View Record in Scopus Google Scholar - SN Papageorgiou, D Koletsi, A Iliadi, T Peltomaki, T. Eliades
Treatment outcome with orthodontic aligners and fixed appliances: a systematic review with meta-analyses
Eur J Orthod, 42 (2020), pp. 331-343
View PDF CrossRef View Record in Scopus Google Scholar - DL Sackett, WM Rosenberg, JA Gray, RB Haynes, WS. Richardson
Evidence based medicine: what it is and what it isn’t
BMJ, 312 (1996), pp. 71-72
View PDF CrossRef Google Scholar - SH. Miles
Hippocrates and informed consent
Lancet, 374 (2009), pp. 1322-1323
Article Download PDF View Record in Scopus Google Scholar - Hippocrates
The Law: Part 1. The Genuine Works of Hippocrates
Charles Darwin Adams, Dover, New York (1868)
Google Scholar


